You’ve adjusted your diet. You’re walking after meals. Maybe you’re on Metformin. And yet something still feels like it’s missing — like the numbers should be moving faster than they are. For some people, the answer lies in vitamins for insulin resistance — a micronutrient gap that the condition itself creates, and that most doctors never think to check.
Not a magic pill. Not a shortcut. But a real, evidence-based layer worth understanding.
This is what the research actually says. No hype. No brand pushing. Just the mechanisms worth understanding.
Important before you continue: Supplements can interact with medications — including Metformin, blood thinners, and other diabetes drugs. Some on this list have meaningful interactions you need to know about before starting. Please speak to your pharmacist or doctor before adding anything new, especially if you are already on chronic medication.
Why Vitamins for Insulin Resistance Matter
Insulin resistance doesn’t just affect your blood sugar — and if you’re unclear on exactly what insulin does inside your body; What Does Insulin Do to Your Body covers the full mechanism. It creates a cellular environment that actively depletes specific micronutrients — and when those nutrients drop, insulin signalling gets worse.
It’s a cycle. Insulin resistance lowers magnesium. Lower magnesium worsens insulin resistance. The same pattern plays out with Vitamin D, chromium, and omega-3 fatty acids. Furthermore, chronic inflammation — which runs alongside insulin resistance in almost every case — increases the body’s demand for these nutrients faster than food alone can replace them. And if you’ve been wondering whether insulin resistance is behind your weight struggles; Does Insulin Resistance Cause Weight Gain explains the connection directly.
This doesn’t mean supplements replace lifestyle. They don’t. What they can do is fill the gaps that insulin resistance created — and that’s exactly why vitamins for insulin resistance deserve a closer look alongside the lifestyle work you’re already doing.
Magnesium — The Most Common Deficiency Nobody Talks About
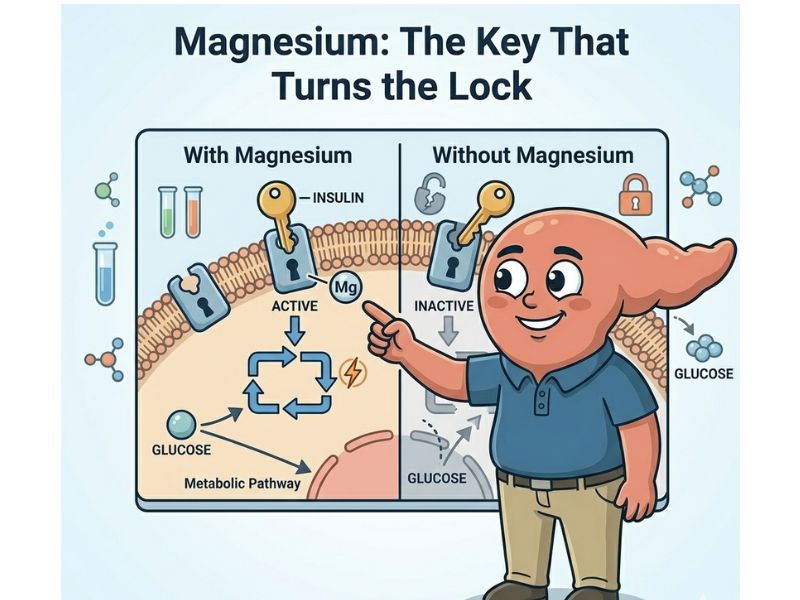
Magnesium is involved in over 300 enzymatic reactions in the body. One of the most important: activating insulin receptors on your cells.
When magnesium is low, insulin knocks on the door — but the lock doesn’t turn properly. Consequently, your pancreas has to produce more insulin to get the same result. That’s the definition of insulin resistance getting worse.
Research consistently shows that people with prediabetes and Type 2 diabetes have lower magnesium levels than metabolically healthy individuals. The deficiency isn’t coincidental. Insulin resistance itself increases magnesium excretion through the kidneys — meaning the worse your insulin resistance, the more magnesium you lose.
Chronic stress compounds this further — if you haven’t read; Does Stress Affect Blood Sugar, the cortisol connection is worth understanding.
Food sources include dark leafy greens, pumpkin seeds, almonds, and dark chocolate. However, if your gut health is compromised or your diet is still a work in progress, food sources alone may not close the gap.
Supplementation: Magnesium glycinate or magnesium citrate are the best-absorbed forms. Magnesium oxide — the cheapest version on most pharmacy shelves — absorbs poorly. Worth knowing before you buy.
Vitamin D — The Deficiency Worth Checking First
Vitamin D is technically a hormone precursor. Your pancreatic beta cells — the ones that produce insulin — have Vitamin D receptors on them, and Vitamin D deficiency is consistently associated with impaired insulin secretion and increased insulin resistance in observational studies.
However, the evidence for supplementation is more nuanced than it first appears. A large, well-controlled 2022 trial involving over 2,000 people with prediabetes found that Vitamin D supplementation did not improve insulin sensitivity or beta-cell function for the group as a whole. A benefit was only observed in participants who were severely deficient at the start of the study.
What this means practically: if your Vitamin D levels are already adequate, supplementing more won’t move the needle on insulin resistance. But if you’re genuinely deficient — which is more common than most people assume — correcting that deficiency matters.
In South Africa, low Vitamin D levels are more common than expected. Skin tone, sunscreen use, time of day, gut absorption, and obesity all reduce how much you actually convert from sun exposure. Adipose tissue sequesters Vitamin D, making it biologically unavailable even when blood levels appear normal.
The starting point is a blood test, not a supplement. Ask your doctor for a 25-hydroxyvitamin D test. If deficiency is confirmed, correcting it is worthwhile.
Supplementation: Vitamin D3 is the preferred form. It’s best taken with Vitamin K2, which directs calcium to bones rather than arteries. This combination matters — more on that when we look at the full stack later in this series.
Berberine — The Plant Compound That Surprises Doctors
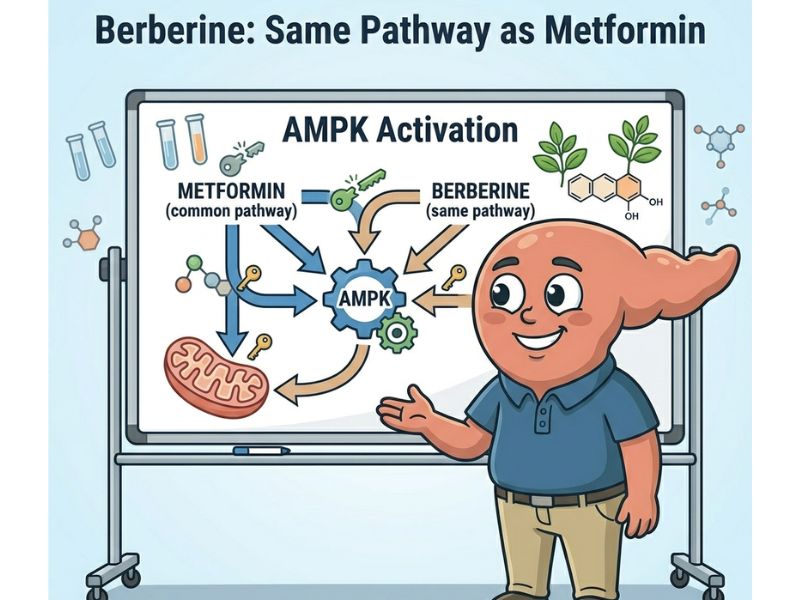
Berberine is a bioactive compound found in several plants — goldenseal, barberry, and others. It activates an enzyme called AMPK — the same metabolic pathway that Metformin targets.
That comparison gets attention in research circles for good reason. Several studies have shown berberine producing blood sugar improvements comparable to Metformin in people with Type 2 diabetes. Furthermore, it appears to improve insulin sensitivity, reduce fasting glucose, and lower HbA1c.
That said, this is not a reason to swap your Metformin for berberine without medical supervision. It is a reason to take the evidence seriously.
Critical interaction warning: Berberine affects liver enzymes — specifically the CYP450 system — that process many common medications, including some antidepressants, statins, blood pressure drugs, and blood thinners. This is not just a diabetes-medication issue. If you are on any chronic medication, speak to your pharmacist before adding berberine. Additionally, if you are on Metformin, combining berberine can theoretically cause blood sugar to drop too low — though documented cases are uncommon. The CYP450 interaction is the broader and more clinically significant concern.
Chromium and Alpha-Lipoic Acid — The Supporting Players
Chromium potentiates insulin signalling — meaning it helps insulin do its job more efficiently at the receptor level. The mechanism is plausible and well-described. However, the research is mixed. Some studies show modest benefit; others show none. It would not be the first or second supplement to add, and for many people, it may not be worth the money until the higher-priority gaps are addressed first.
If you do try chromium, picolinate is the most studied form. Doses used in research typically range from 200–400mcg daily. Discuss the right dose with your pharmacist or doctor before starting.
Alpha-lipoic acid (ALA) has stronger evidence for insulin sensitivity than chromium, particularly in people with prediabetes and Type 2 diabetes. It’s an antioxidant that improves glucose uptake and reduces oxidative stress — both relevant to insulin resistance. The dose used in most research is 600mg daily. ALA is generally safe, but it can lower blood sugar and may interact with thyroid or cancer medications. Discuss with your pharmacist or doctor first.
Omega-3 — The Anti-Inflammatory Foundation
Omega-3 fatty acids — specifically EPA and DHA — don’t directly lower blood sugar. What they do is reduce the chronic low-grade inflammation that underlies insulin resistance in the first place.
The modern diet is heavily skewed toward omega-6 fatty acids — found in seed oils, processed foods, and grain-fed meat. Omega-6 promotes inflammation. Omega-3 counters it. When the ratio tips too far toward omega-6, the inflammatory environment makes insulin resistance harder to reverse.
Similarly, omega-3s support cell membrane fluidity — which affects how well insulin receptors function. Stiff, inflamed cell membranes don’t respond to insulin the way healthy ones do.
This is the entry point to a much deeper conversation about inflammation, gut health, and the LPS cycle — which we’ll cover in full in a later blog article. For now, the bottom line is this: omega-3 is the anti-inflammatory foundation that makes everything else work better.
To be clear: omega-3s don’t directly lower blood sugar in most people. The benefit is anti-inflammatory, which helps create the conditions where insulin sensitivity can improve. That means omega-3s matter most in people carrying significant chronic inflammation — which, in the context of insulin resistance, is most people.
Supplementation: Look for IFOS or GOED-certified fish oil — these are third-party quality standards that confirm purity and EPA/DHA content. Dose matters: 2–3g of combined EPA+DHA daily is the range used in most metabolic research. Most standard capsules contain far less than the label implies — many products need 4–6 capsules to reach 2g. Read the small print before you buy.
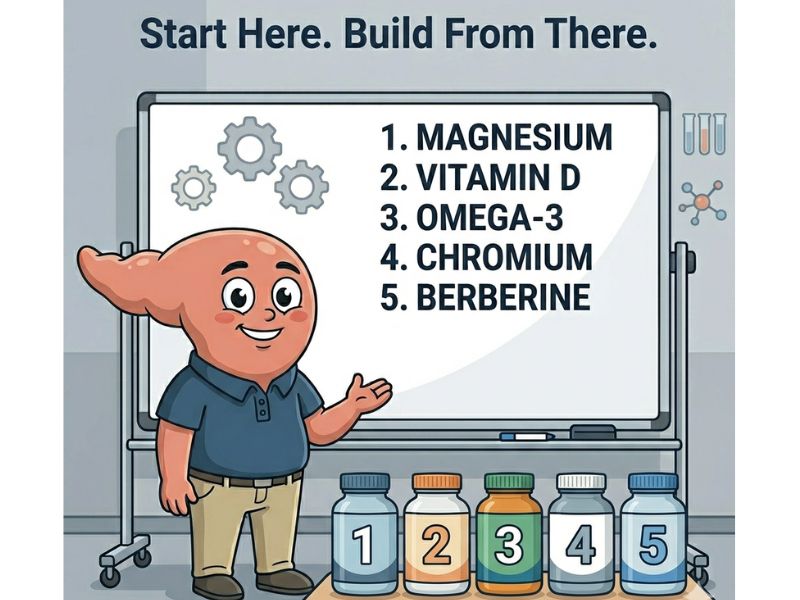
The Best Vitamins for Insulin Resistance — Ranked by Evidence
Not all supplements are equal. Here’s the priority framework based on evidence strength and relevance to insulin resistance specifically:
1. Magnesium — highest relevance, most common deficiency, direct insulin receptor mechanism
2. Vitamin D3 + K2 — strong deficiency link, beta cell function, widely under-tested
3. Berberine — strongest blood sugar evidence, requires pharmacist guidance if on medication
4. Omega-3 — anti-inflammatory foundation, essential for the full protocol
5. Chromium — supporting role, fills a specific gap, low risk
This is not a shopping list. It’s a priority framework. Start with the most likely deficiency — for most people with insulin resistance, that’s magnesium and Vitamin D — and build from there.
Supplements are one layer. But insulin resistance runs deeper than a micronutrient gap — it affects how your body handles stress, food, movement, and recovery. Your Body Is Talking: A Pharmacist’s Guide to Stopping Prediabetes covers the full picture. It’s free.
How These Vitamins Support Insulin Sensitivity Together
None of these work in isolation. Magnesium supports the insulin receptor. Vitamin D supports the beta cell. Berberine activates the same pathway Metformin uses. Omega-3 reduces the inflammation that makes all of the above harder. Chromium helps insulin signal more efficiently.
In other words, they address different parts of the same problem. That’s why the evidence for each one individually understates what they can do together — when lifestyle is already in place.
That last part matters. These supplements amplify what’s already working. They don’t replace the walk after supper — and if you’re not doing that yet; Walking After Eating: 15 Minutes That Lower Blood Sugar is the place to start.
They don’t replace the reduction in refined carbohydrates — and Foods to Reverse Prediabetes covers that ground in full. What they do is remove biochemical obstacles that lifestyle alone can’t always clear.
Vitamins for Insulin Resistance vs Medication
This is not a choice between supplements and medication. For most people, it’s not either-or.
If you’re on Metformin, that medication is doing a specific job — and doing it well. These supplements support insulin sensitivity through different mechanisms. They are not a replacement. They are a complement.
That said, if you’ve been managing prediabetes for a while and feel like you’ve hit a ceiling despite doing the right things — a micronutrient check is a conversation worth having with your doctor or pharmacist. A simple blood test can confirm Vitamin D and magnesium status. From there, the gaps become visible.
Vitamin B12 — The One Metformin Takes Away
This one doesn’t improve insulin sensitivity. But if you’re on Metformin, it belongs in this conversation.
Long-term Metformin use reduces B12 absorption in the gut — and studies suggest 20–30% of long-term users develop a deficiency over time. The symptoms are easy to miss: fatigue, numbness or tingling in the hands and feet, and brain fog. The problem is that those symptoms look exactly like diabetic neuropathy — which means many people are treated for the wrong thing.
If you’ve been on Metformin for more than a year, ask your doctor for a B12 blood test. Deficiency is correctable. Oral B12 supplements at higher doses — 1000mcg or more — can work despite Metformin’s effect on absorption, though your doctor may recommend a specific form based on your blood levels. The key is knowing the deficiency exists first.
How to Use These Vitamins for Insulin Resistance Safely
Using vitamins for insulin resistance effectively comes down to a few practical rules:
Get tested before you start where possible. For Vitamin D and magnesium — and B12 if you’re on Metformin — blood testing is inexpensive and widely available. Ask your doctor for a serum magnesium and 25-hydroxyvitamin D test. One important nuance: serum magnesium can appear normal even when tissue magnesium is low. A normal result doesn’t automatically rule out deficiency — which is another reason to have the conversation with your pharmacist rather than relying on the number alone.
Start one at a time. If something causes a reaction — digestive upset, unusual fatigue, blood sugar changes — you need to know which supplement caused it. Adding three at once makes that impossible.
Check your current medications first. Berberine and Metformin is the highest-risk combination on this list. But Vitamin D can also interact with certain heart and kidney medications. Your pharmacist can check your full medication list in under five minutes.
Quality matters more than price. Cheap supplements often contain poorly absorbed forms — magnesium oxide, cheap chromium chloride, fish oil that’s already oxidised. The form matters as much as the dose.
Give it time. Micronutrient correction takes weeks, not days. Don’t expect blood sugar changes overnight. Expect them over months — alongside everything else you’re already doing.
The Bottom Line : Vitamins for Insulin Resistance
Insulin resistance doesn’t just resist insulin. It depletes the very nutrients your cells need to respond to it properly. That depletion isn’t a character flaw — it’s a biochemical consequence of the condition itself.
Filling those gaps — with the right forms, in the right order, alongside lifestyle — is not grasping at shortcuts. It’s being thorough. It’s a piece of the picture that many people never learn about because nobody told them it existed.
Start with magnesium and Vitamin D. Talk to your pharmacist or doctor. Build from there.
The body is talking. This is part of what it’s saying.
Want to understand what’s driving your insulin resistance beyond the nutrient gaps? The free ebook covers the stress-sugar connection, the patterns most people miss, and a practical 30-day starting point.
[Get the Complete Guide Free →]
Medical Disclaimer: The information on this website is for educational purposes only and is not intended as medical advice. Always consult your doctor or pharmacist before making changes to your medication, supplement routine, or lifestyle — especially if you have a chronic condition or are on chronic medication.
References:
- Omega-3 Sinha et al. (2023) — The Effect of Omega-3 Fatty Acids on Insulin Resistance https://pubmed.ncbi.nlm.nih.gov/37374105/ PMC full text: https://pmc.ncbi.nlm.nih.gov/articles/PMC10305526/
- Vitamin D3 Xu et al. (2022) — Association between vitamin D3 levels and insulin resistance: a large sample cross-sectional study https://pubmed.ncbi.nlm.nih.gov/34997087/ PMC full text: https://pmc.ncbi.nlm.nih.gov/articles/PMC8741779/
- Magnesium — Rodríguez-Morán & Guerrero-Romero (2003) — Oral magnesium supplementation improves insulin sensitivity and metabolic control in type 2 diabetic subjects https://pubmed.ncbi.nlm.nih.gov/12663588/