Inflammation and insulin resistance.
You have adjusted your diet. And you are walking after meals. You are taking your medication. And yet the numbers are not moving the way they should.
If that is where you are, there is something worth understanding — something most people managing prediabetes have never had properly explained. Not another diet tip. Not another reminder to exercise more. Something upstream. Something running silently in the background that works against every effort you are making.
That something is chronic inflammation. And its relationship with insulin resistance is one of the most important — and most overlooked — conversations in metabolic health.

Important before you continue: Some of the dietary and lifestyle changes discussed in this blog — particularly around omega-3 supplementation and anti-inflammatory eating — can interact with existing medications, including blood thinners and Metformin. If you are on chronic medication, please speak to your pharmacist or doctor before making significant changes to your diet or supplement routine.
What Inflammation and Insulin Resistance Actually Have in Common
When most people hear the word inflammation, they think of something visible. A swollen ankle. A red, painful cut. The heat around a bruise. That kind of inflammation is acute — it arrives fast, does its job, and clears.
Chronic inflammation is different. It is low-grade. Persistent. There is no obvious swelling, no visible redness, no dramatic signal. It runs quietly in the background, producing a steady stream of inflammatory molecules called cytokines — chemical messengers your immune system uses to coordinate its response.
The problem is that those same cytokines interfere with something you need to work properly: insulin signalling.
Insulin is the hormone that unlocks your cells and allows glucose to enter. When inflammatory cytokines are circulating at chronically elevated levels, they begin to disrupt the way your cells respond to insulin’s signal. The lock gets harder to turn. Glucose stays in the bloodstream longer than it should. Your pancreas compensates by producing more insulin to force the process. Over time, the demand increases and the system strains under the load.
That is insulin resistance — and inflammation is one of the mechanisms quietly driving it. For a deeper explanation of what insulin actually does inside your body, the full mechanism is covered in detail separately.
Why Your Cells Stop Listening to Insulin
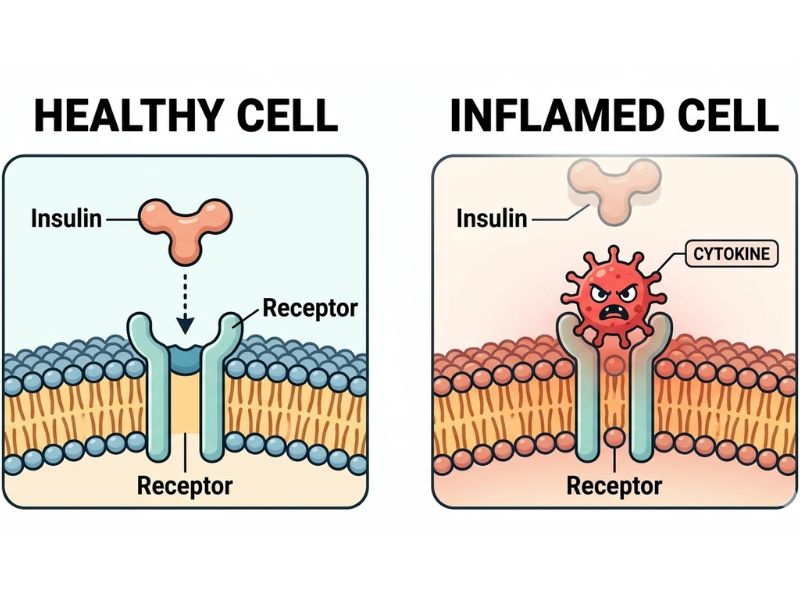
Two cytokines appear consistently in the research on inflammation and insulin resistance: TNF-α (tumour necrosis factor alpha) and IL-6 (interleukin-6). Both are produced in response to chronic inflammatory signals. Both interfere directly with insulin receptor function.
When these cytokines bind to cell receptors, they trigger a chain of molecular events that block the insulin signalling pathway. Specifically, they interfere with a protein called IRS-1 — insulin receptor substrate 1 — which is an essential step in the process of glucose uptake.
In plain language: the inflammatory signal tells the cell to ignore insulin. The cell complies. Glucose accumulates. The pancreas pushes harder. The cycle begins.
The Cycle Nobody Explains
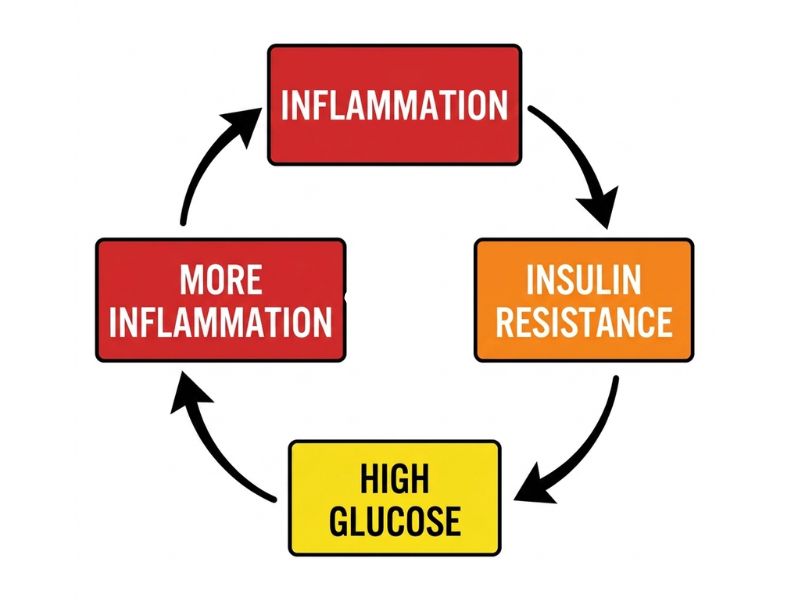
Here is what makes chronic inflammation particularly difficult to manage: it does not just contribute to insulin resistance. Insulin resistance, in turn, drives more inflammation. The two conditions feed each other in a loop that tightens with every rotation.
Elevated blood glucose generates oxidative stress — a byproduct of glucose metabolism that damages cells and triggers further immune response. That immune response produces more cytokines. More cytokines worsen insulin signalling. Blood glucose rises further. The loop continues.
This is why numbers plateau. Not because effort has failed — but because the environment the effort is working inside has not changed. Addressing diet and exercise without addressing the inflammatory load is like bailing water from a boat with a slow leak. The bailing matters. But so does the leak.
Sugar’s specific contribution to this inflammatory load is worth understanding separately — it operates through a slightly different mechanism and compounds the cycle in its own right.
How Inflammation and Insulin Resistance Feed Each Other

Visceral fat — the fat stored around your abdominal organs — plays a significant role in this cycle. Unlike subcutaneous fat stored just beneath the skin, visceral fat is metabolically active. It produces and releases cytokines directly into the bloodstream, functioning almost like an inflammatory organ in its own right.
More visceral fat means more circulating cytokines. More cytokines mean worse insulin signalling. Worse insulin signalling means more glucose stored as fat — and more fat produced. The loop tightens with every rotation.
This is not a character observation. It is not about willpower or discipline. It is biology — a self-reinforcing loop that requires a different kind of intervention than motivation alone can provide.
The Gut Connection
There is a third driver in this picture that receives very little attention in standard prediabetes conversations — and it may be the most upstream of all.
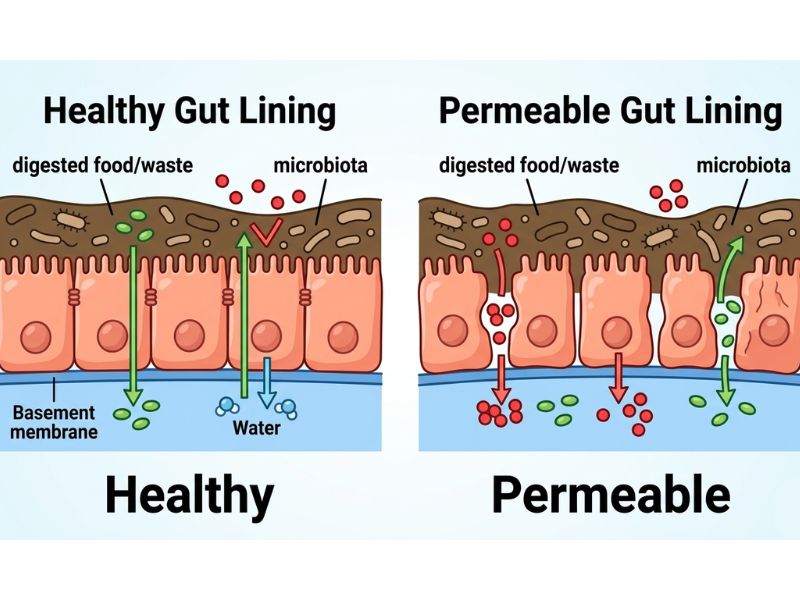
Your gut lining is a selective barrier. When it is healthy, it allows nutrients through while keeping harmful substances — including bacterial components — contained within the digestive tract. When that barrier is compromised, it becomes permeable. Things that should stay inside begin to leak through.
One of those things is lipopolysaccharide — LPS for short. LPS is a molecule found on the outer membrane of certain gut bacteria. Under normal conditions, it stays in the gut where it belongs. When the gut lining is damaged or permeable, LPS enters the bloodstream.
Your immune system recognises LPS immediately as a threat. It responds with an inflammatory cascade. Cytokines are released. Systemic inflammation rises. And because that inflammation interferes with insulin signalling — as described above — blood glucose follows.
This is the mechanism behind what is sometimes called leaky gut. And it is one of the reasons two people can follow the same dietary changes and get very different results. The state of the gut barrier is a variable most standard conversations about prediabetes never address.
Leaky Gut and Insulin Resistance — The Link Most People Miss
What damages the gut lining in the first place? The research points consistently to a cluster of factors that overlap almost entirely with the lifestyle patterns associated with prediabetes and metabolic dysfunction.

Ultra-processed food disrupts the gut microbiome and weakens the gut barrier over time. Excess refined sugar feeds bacteria that produce inflammatory metabolites. Chronic stress compromises the gut lining directly — through cortisol’s effect on gut motility and permeability — and its effect on blood sugar runs deeper than most people realise. Alcohol — particularly in higher or frequent amounts — increases gut permeability measurably; even moderate intake has been shown to have this effect acutely, and what alcohol actually does to blood sugar follows a similarly underappreciated mechanism.
The gut is not a separate system. It is part of the same inflammatory environment — and addressing it is part of breaking the cycle.
What Breaks the Cycle of Inflammation and Insulin Resistance

The answer is not a single supplement. It is not one dietary swap. It is a reduction in the overall inflammatory load — through several levers applied consistently over time.
The foundation is food. An anti-inflammatory eating pattern is not a restrictive protocol. It is a shift toward whole, minimally processed foods — vegetables, legumes, fatty fish, olive oil, nuts, and seeds — and away from the ultra-processed, high-sugar, high-refined-carbohydrate patterns that drive both gut damage and systemic inflammation. The less processed the food environment, the less the immune system is provoked.
Movement is the second lever. Physical activity reduces circulating inflammatory cytokines directly — not through weight loss alone, but through the anti-inflammatory effect of muscle contraction itself. Short, consistent movement is more effective than occasional intense effort, and walking after eating remains one of the most accessible and evidence-supported entry points.
Sleep is the third. Chronic sleep deprivation elevates inflammatory markers measurably — including CRP, IL-6, and TNF-α — and the relationship between sleep and blood sugar makes clear that addressing sleep is not optional when inflammation is part of the picture.
Where Omega-3 Fits Into the Inflammation Picture
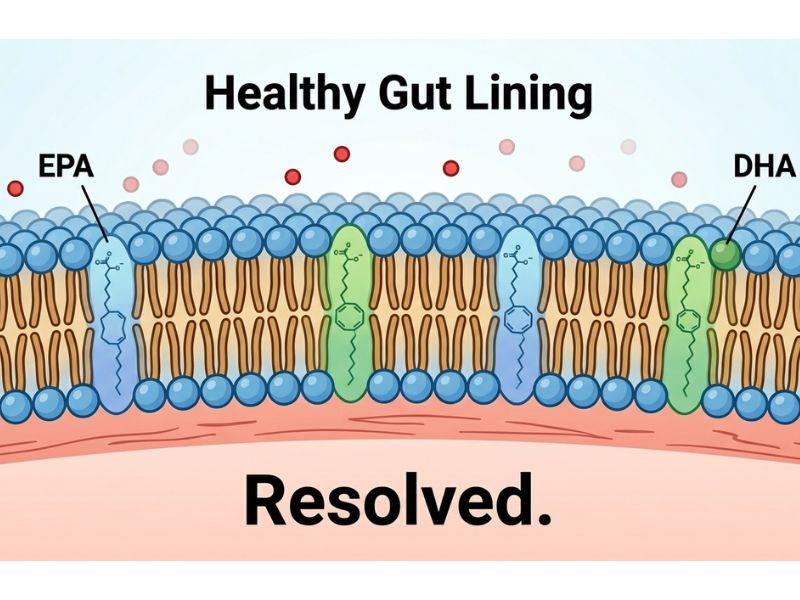
Once the foundation is in place, omega-3 fatty acids — specifically EPA and DHA — offer a targeted mechanism for reducing the inflammatory environment further.
EPA and DHA are incorporated into cell membranes throughout the body. They are the precursors for a class of anti-inflammatory molecules called resolvins and protectins — compounds that actively resolve inflammatory responses rather than simply suppressing them.
In the context of insulin resistance specifically, omega-3 supplementation has been shown to reduce circulating TNF-α and IL-6 levels, improve cell membrane fluidity, and enhance insulin receptor sensitivity. The effect is not dramatic in isolation. But as part of a broader reduction in inflammatory load, it is meaningful.
The full mechanism — including what to look for in a supplement and what the research actually shows — is covered in Omega-3 and Blood Sugar.
What the Research Says About Inflammation and Insulin Resistance
The evidence connecting chronic inflammation to insulin resistance is not new or contested. It has been accumulating for over two decades.
A landmark study published in Cell Metabolism demonstrated that inflammatory cytokines directly impair insulin receptor substrate signalling — the molecular mechanism described earlier. Subsequent research has confirmed that elevated hsCRP (high-sensitivity C-reactive protein) — a standard inflammatory marker — is consistently associated with increased risk of Type 2 diabetes progression in people with prediabetes.
The LPS-insulin resistance connection has been confirmed in multiple human studies, including research published in PLOS ONE showing that endotoxemia — elevated LPS in the bloodstream — is independently associated with insulin resistance even when other variables are controlled.
Furthermore, omega-3 intervention trials have demonstrated measurable reductions in inflammatory cytokines in people with metabolic syndrome, with corresponding improvements in insulin sensitivity markers.
The science is not theoretical. The mechanisms are established. What is missing is the conversation — the explanation that connects these dots for the person sitting with a prediabetes diagnosis and numbers that are not responding.
What This Means for Your Numbers
If your blood glucose is elevated despite genuine effort, inflammation may be the variable that has not yet been addressed.
Not the only variable. But a real one. One that operates upstream of diet and exercise — in the cellular environment where insulin either works or doesn’t.
The cycle is real. It is also breakable. Not through a single intervention, but through a systematic reduction of the inflammatory load — in the food environment, the gut, the stress response, the sleep pattern, and the supplement layer where appropriate.
How to Know If Inflammation Is Affecting Your Insulin Resistance
There is one test worth asking your doctor about: hsCRP — high-sensitivity C-reactive protein. It is a standard blood marker for systemic inflammation. Elevated levels in the context of prediabetes suggest that inflammation is active in the picture.
Fasting insulin is a second useful marker — not always included in standard prediabetes panels, but worth requesting. Elevated fasting insulin alongside elevated glucose is a strong signal that insulin resistance is driving the picture.
Waist circumference remains one of the most practical proxies. Visceral fat is an inflammatory organ. A waist measurement above 94cm in men or 80cm in women is associated with elevated metabolic and inflammatory risk in South African populations.
None of these are diagnostic conversations — they are awareness conversations. If your numbers are plateauing and you have not checked these markers, it is worth raising with your doctor or pharmacist at your next visit.
The Bottom Line

Inflammation is not a side issue in prediabetes. It is a central driver — one that runs silently, interferes with insulin signalling at a cellular level, and creates a cycle that effort alone cannot fully break.
You are not failing. The environment is working against you. Environments can be changed.
The next step in this series looks at the specific vitamins and minerals that support insulin sensitivity — starting with the ones most commonly depleted by insulin resistance itself. That conversation continues in Vitamins for Insulin Resistance: What Actually Works.
Medical Disclaimer
The information in this blog is for educational purposes only and does not constitute medical advice. Always consult your doctor or pharmacist before making changes to your medication, diet, or supplement routine. Individual results vary. This content is intended for adults with prediabetes or those at risk of Type 2 diabetes and is not a substitute for professional medical care.
References
- Liang H, et al. (2013). Effect of Lipopolysaccharide on Inflammation and Insulin Action in Human Muscle. PLOS ONE, 8(5), e63983. https://pmc.ncbi.nlm.nih.gov/articles/PMC3660322/
- Cai D, et al. (2005). Local and systemic insulin resistance resulting from hepatic activation of IKK-β and NF-κB. Nature Medicine, 11, 183–190. https://pmc.ncbi.nlm.nih.gov/articles/PMC1440292/